Medical laboratory workshop Episode 7: What does differential white blood cell count say about your health condition?
It's another lovely day and I remain your favourite host for this interesting series of medical workshop. In our previous episode, we looked at white blood cell count and their significance in diagnosis of a disease condition.
Today, I intend to step up the last article to the more definitive form of it by elaborating more about differential white blood cell count and how they give more detailed information about the state of ones health or disease condition.
Do you wish, to understand white blood cell count and its relevance in diagnosis, feel free to read this article - medical laboratory workshop episode 6: babys death due to negligence by parents.
Besides the medical knowledge you will gain, you will also get to understand human behaviour and some reasons why people act or do things. That aside, let's get on real quick with our discussion for today, and as usual, we begin with an introduction to the concept of differential white blood cell count.
Introduction
The human blood is made of different cells that operate in unison to ensure and maintain stability and physiologic functions in the human body system. Most of these cells operate and function within the confines of the human circulatory system, carrying nutrients, minerals, hormones, protein, oxygen etc. to organs and tissues that have need for them and at the same time, carrying waste and toxic metabolites to organs like the kidney for excretion out of the body in the form of urine or to the intestine as stool.
In disease condition, the functionality of these cells could be hampered and as a result, can lead to serious challenge in maintaining the normal homeostasis and internal body millieu (internal body environment). In some conditions, the blood cells can either be elevated or reduced drastically. Estimation of the cells number and comparing them to the normal reference range, helps the physician in understanding the pattern of the disease or the etiology.
We will carefully study each blood cells and discuss their variations in different disease conditions. Basically, the major blood cells include the White cells (Neutrophils, eosinophils, basophils, lymphocytes and monocytes) and platelets, and red blood cells (erythrocytes). Just like I earlier said, their variation is dependent on the type of infection.
For example, in parasitic infections, the major cells are known to elevate are the eosinophils while in bacterial infections, you would expect to see more of the neutrophils in the blood circulation.
Having an idea of this gives you an immediate idea of what you are up against in the patient and hence, it will guide your treatment pattern but this is not used in isolation, a view of the blood film gives a more definitive diagnosis. In essence, differential blood cell count is complemented by blood film results.
Differential white blood cell count using EDTA tube
{kind=link}
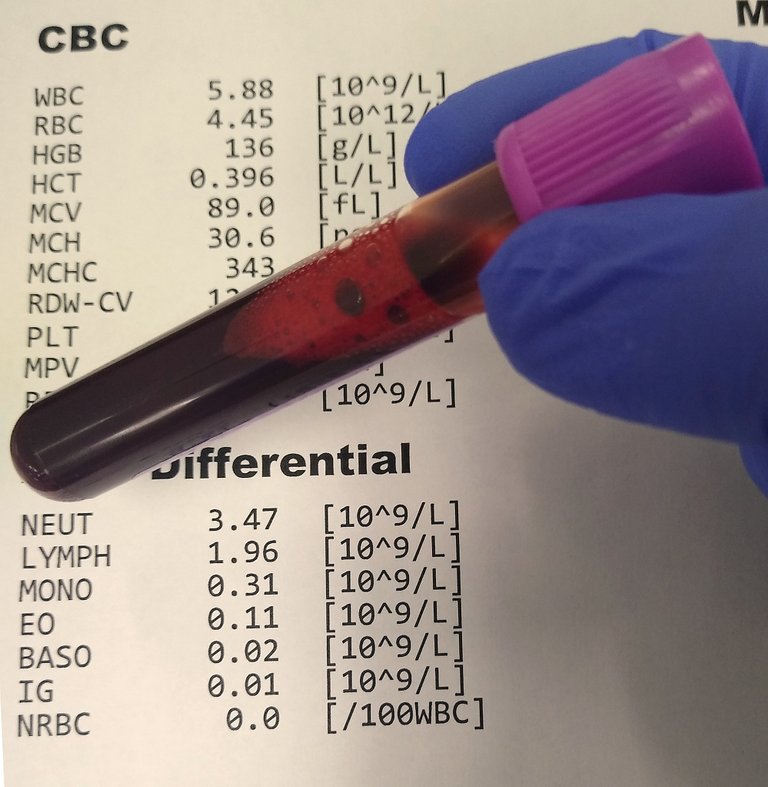
Usually when investigations are to be done, in most cases, the standard protocol is to request for a Complete blood cell count (CBC) aka Full blood count (FBC). Full blood count (FBC) is made up of White blood cell count (WBC) and its differentials, Red blood cells count, platelet count, Haemoglobin (estimates the concentration of the protein responsible for carrying oxygen), Haematocrit (estimates the percentage of red blood cells in an individual).
Others include the red cell indices. These values are derived from the values of the above and then calculated. Red cell indices include the Mean corpuscular volume (MCV), Mean corpuscular hemoglobin (MCH), Mean corpuscular hemoglobin concentration (MCHC), Mean platelet volume (MPV), Red cell distribution width (RDW). Red cell indices helps in understanding the real cause of anaemia in a patient.
For instance, with the values gotten from MCV (indicates the size of the red blood cells), when they are high, it means that the patient is probably lacking vitamin B12 or suffering from folate deficiency. This type of anaemia is referred to as Megaloblastic anaemia. If the value is lower than normal, it means the red cells are smaller in size, hence the patient would likely be suffering from iron deficiency anaemia aka Microcytic anaemia.
MCH on the other hand measures the amount of haemoglobin in an average red blood cell in an apparently healthy adult and it is measure in picograms while MCHC measures the average hemoglobin concentration in a volume of blood and it is calculated in percentage. MPV estimates the size of the platelets while RDW measure the variations in the erythrocyte sizes.
Automated full blood cell Counter
{kind=link}
FBC count is easily done with an automated blood cell Counter and they give more accurate results of blood cells. However, these results sometimes are not enough because, it does not reveal the shapes and sizes of the blood physically.
Take for instance, an automated blood cell counter cannot detect sickle cells. Sickle cells are better seen when a blood film is made and then stained. A blood film helps us characterize and understand the morphology and sizes of the red blood cells.
In situation where you have excessive variation in the size of the red blood cells, this condition is refered to as Anisocytosis. This could be cause by microcytic anemia if the cells are smaller or Megaloblastic anemia if the cells are excessively larger.
It could also be as a result of drugs actions. Anisocytosis is usually interpreted along side RDW because they both measure the size of the red cells. In essence, the results from the blood film should tally with those gotten as RDW from the automated counting machine.
There are situations where there could be errors in the results produced from the counting machine. These error most times are caused by humans. For example, using a sample that has any form of clot in it will give a false result of Haematocrit or packed cell volume.
All the details explained so far above are associated with the red blood cells. When it comes to the white blood cell count, we will be looking more into, the differential count. Differential white blood cell count is made up of (Neutrophils, eosinophils, basophils, monocytes and lymphocytes) and it is done either with the machine or manually. Our focus today will be more on differential white blood cell count.

Blood Cell Counter Five Keys DC Counter
{kind=link}
Differential white blood cell count helps to quantitate the actual number of individual white blood cells in a sample of blood. Usually, values obtained from the automated counter is also supplemented by doing a manual count using the microscope and a differential counter.
Diagnostic procedure
The first step required for differential white blood cell count is to prepare a stained blood film. This is done by placing a drop of blood near the end of the glass slide. Using a spreader positioned at 30-45 degree up to the drop and allow it to spread evenly along the point of contact between the spreader and the glass slide.
The next thing you do is to make a quick but not too fast forward push of the spreader. A good smear will have a feathered tail. Allow the smear to dry well. Fix the smear by dipping it into methanol. This will further increase the adhesion of the cells to prevention washing off. You then stain in any Romanowsky stain (e.g. Leishman, giemsa, May–Grünwald etc.)
The principle behind the staining technique is that, they are generally neutral stains contain methylene blue (azure) dye and Eosin Y. The eosin is an acidic dye that has affinity for basic compounds, hence, it binds to the cytoplasm of a cells giving it a red to pinkish colour while the methylene blue aka azure is basic in nature hence, has affinity for the acidic components of the cell and thus stains the nucleus of the cell purple blue. Let's now take a look at the results.
Results and clinical significance of these cells
Staining of a film be it thick or thin film helps us characterize and identify the type of cells in the blood sample. It reveals the nature and state of the cells and makes it easier to identify and differentiate diseased cells from normal healthy cells. We will reveal all the cells one by one as seen under the microscope. The first is neutrophils.
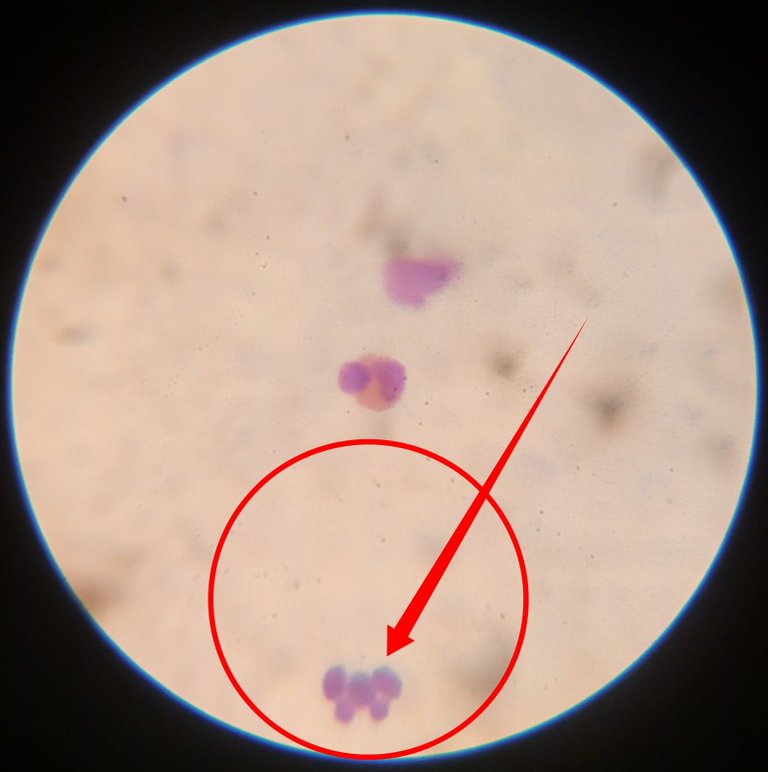
Neutrophils
Neutrophils are also called polymorphonuclear cells because they contain more than one nuclei. They usually have about 3-5 lobes stained purple blue. When they are excessively raised in numbers, it is refered to as neutrophila

During infection, (in most cases bacteria infection) and inflammation, they leave the blood and migrate to the area area affected through a process known as diapedesis. They release inflammatory cytokines aimed at tackling the problem.

In chronic infections, the immature neutrophils are also recruited to fight the infection and this results to the presence of immature neutrophils with bands. This situation is referred to as left shift neutrophila. If the infection is acute or short duration, you tend to see more of the matured neutrophils and this is called right shift neutrophila. They are also seen to be increased in case of appendicitis.

When they are low in number, it could indicate typhoid fever, measles and in cases of infectious hepatitis. Their main function in the body, is to destroy and digest specifically bacteria and fungi during infections. The help facilitate wound healing as quickly as possible, thereby restoring the body's function back to normalcy.
A careful study of these cells will convey a great deal of information about the state of the patient. Our next cell for consideration is the eosinophils.
Eosinophils
Another very important and commonly seen cell is the eosinophils. These cells are usually seen in abundance (eosinophilia) in cases of parasitic infections and even allergic reactions.
They have 2 bilobed nuclei and their cytoplasm stain pink in colour. When they are low in number (eosinopenia) it could be an indication of stress due to increase in the level of corticosteroids.
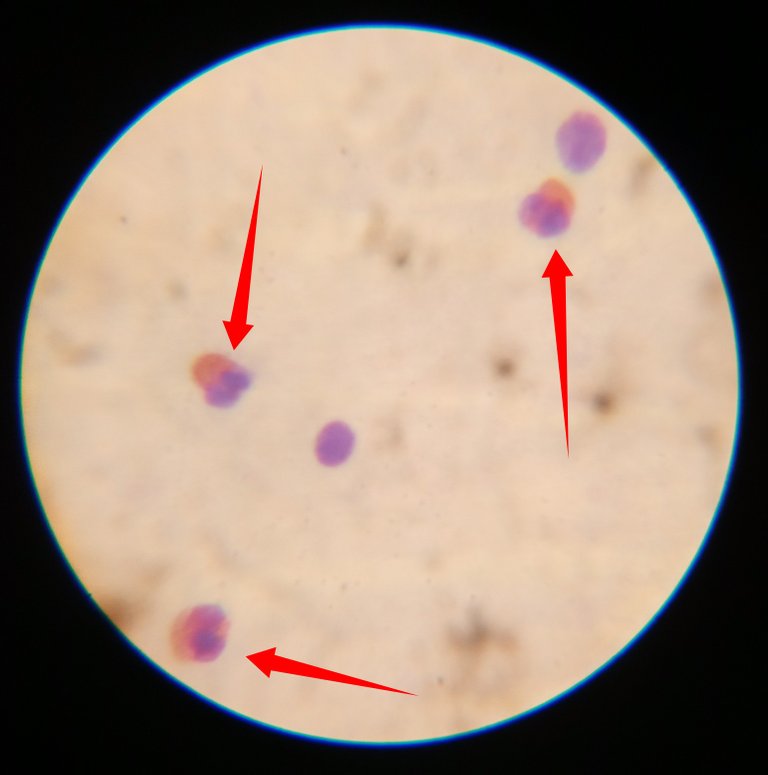
You easily identify them by virtue of their clearly visible pinkish cytoplasm.
The next cell wee will look at is the Lymphocytes. Bear in mind that Neutrophils, Eosinophils and basophils are collectively called granulated cells because their cytoplasm has some granules while lymphocytes and monocytes are referred to as Agranulocytes because they do not have any granules in their cytoplasm.
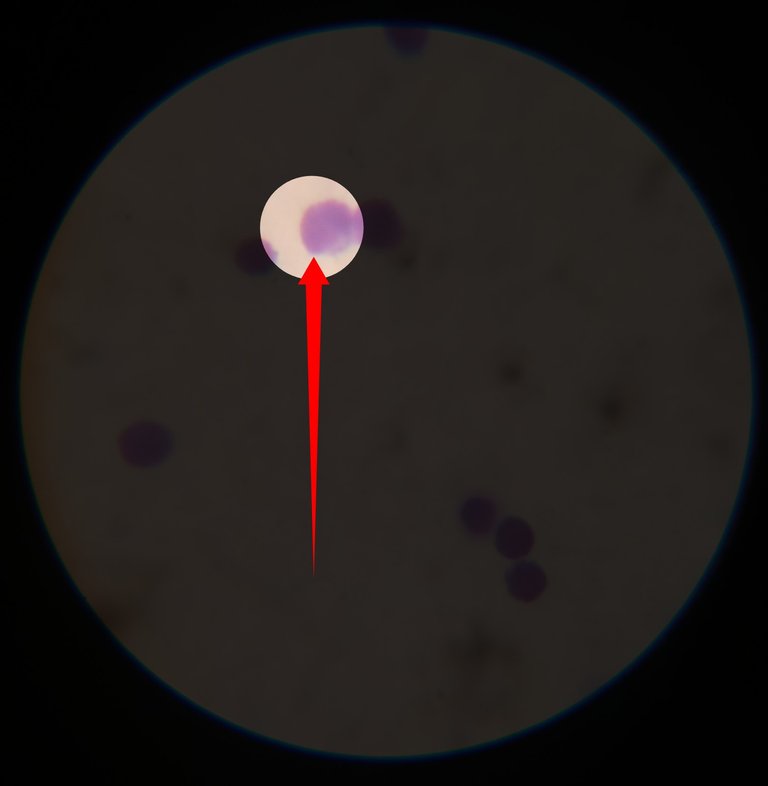
Lymphocytes
Lymphocytes belongs to the category of agranulocytes and they only have just one nuclei within their cytoplasm.
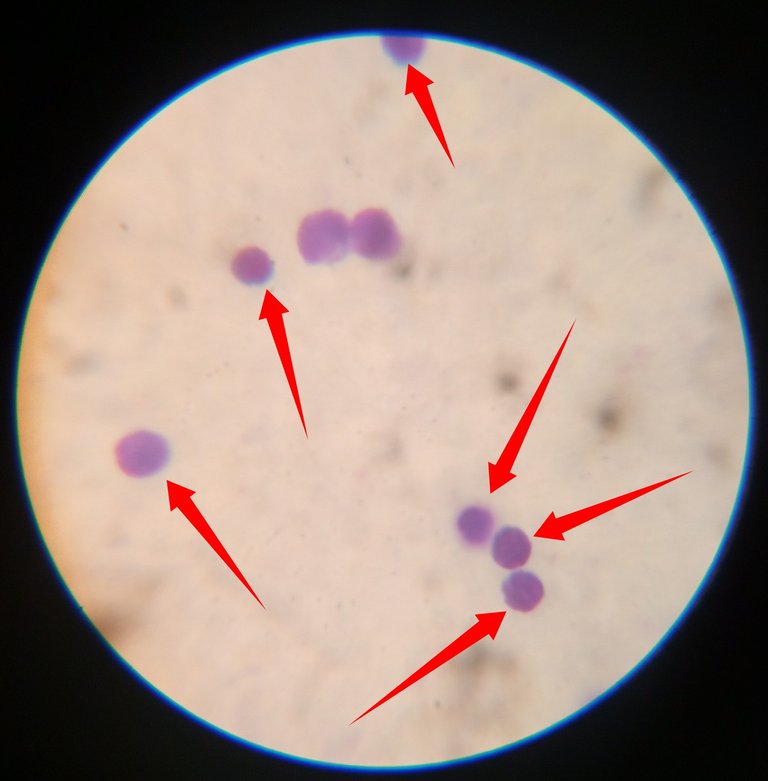
Their nuclei in most cases almost fills their cytoplasm, thus making it a little bit difficult to distinguish them from monocytes which have a bean or kidney shaped nuclei.
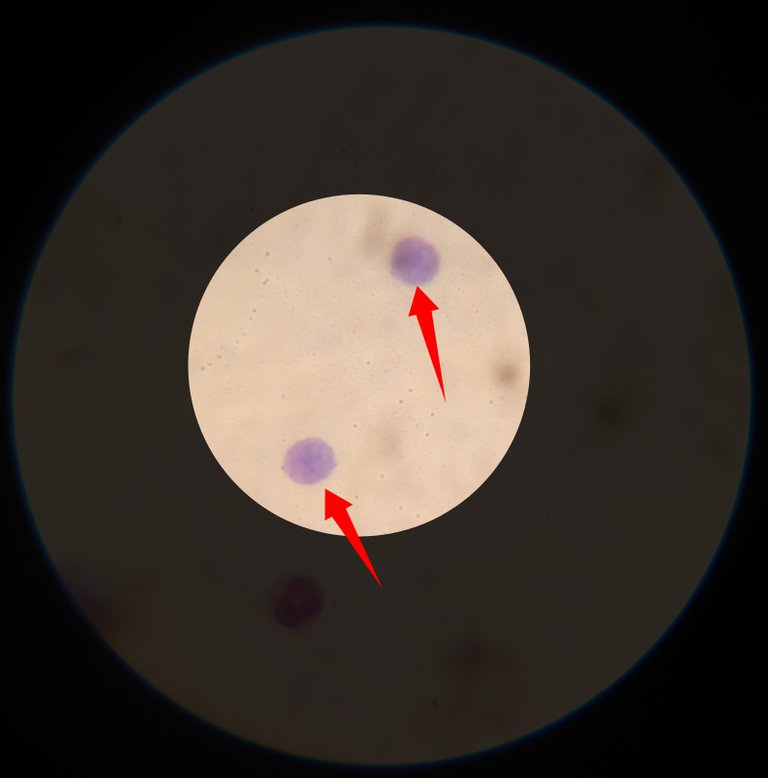
Lymphocytes are seen to be elevated (lymphocytosis) in cases of viral infections. Sme of them can be very large while some are small. When they are low in number, it could be caused by disease's like HIV)AIDS, tuberculosis, hepatitis and chemotherapy. Some auto immune diseases can also cause reduction in the number of lymphocytes in the blood.
The remaining two white cells basophils and monocytes represent the lowest in most cases. Basophils sometimes are usually not present in blood film. They are rarely seen and even though seen, they are very few in number. From all the fields viewed, no basophil was found, so we conclude with monocyte.
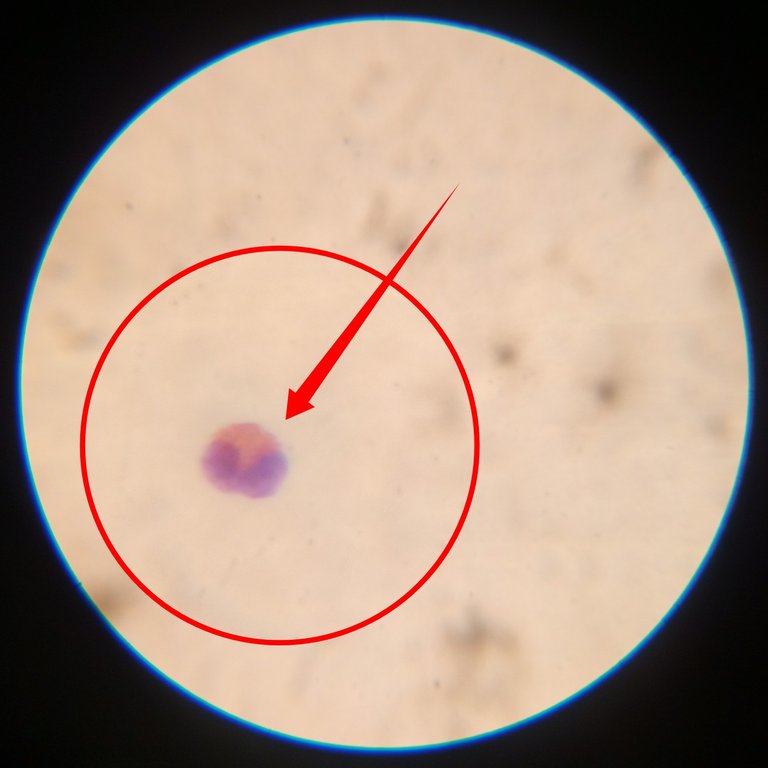
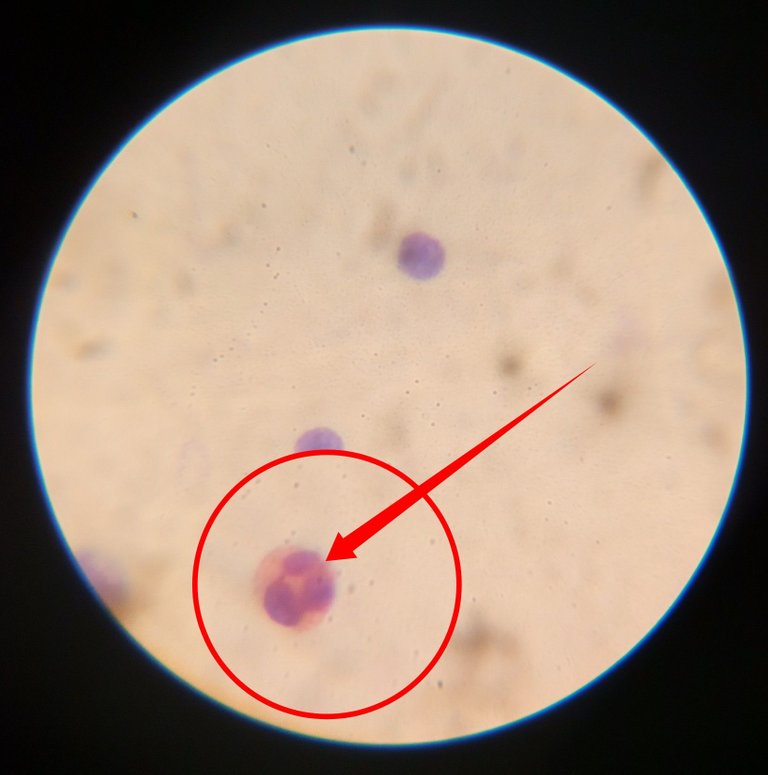
Monocytes
Monocytes generally have a bean like shaped nuclei. It also takes the shape of horse shoe or kidney shape. When they are excessively elevated, it is referred to as monocytosis.
The major indication where you see drastic elevation in the number of monocytes is cancer (leukaemia). It is also seen to be elevated in cases of tuberculosis, chronic inflammation and also in viral infections like measles and mumps.
In conclusion, these cells are very important in diagnosis of some diseases when used in conjunction with other biomedical parameters. Differential white blood cell count is a very important analysis in diagnosis and most never be under estimated.
Until I come your way again, stay awesome!
References
•Chapter 152 Red Cell Indices
•Complete Blood Count (CBC) Test
•DPDx - Laboratory Identification of Parasites of Public Health Concern
•Complete Blood Count (CBC) Test and Results
•What to Know About Neutrophils
•Blood Laboratory
Thank you @cyprianj for constantly giving me content and something informative to read on. I will save this post in my documents, it'll come in handy someday. The truth is, during my training in school to become a nurse, we are never taught deeply on these stuff so in the hospital interpreting test or laboratory results can be challenging. Thank you for this. I'm truly grateful❤️
Sometimes it takes more exposure and experience to fully understand those jargons taught back then in university days.
I would say, your challenge is not different from mine when I newly underwent 1 year internship, but with time and more experience, it becomes easily comprehensible.
Thanks for the read 💖
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider delegating to the @stemsocial account (85% of the curation rewards are returned).
Thanks for including @stemsocial as a beneficiary, which gives you stronger support.
❤️
A simple vial of blood (or probably several!) can reveal so much. I think an article like this can serve as a ready reference for anyone who gets a blood test. Often we can get a printout of the results. (Sometimes we have to ask for that). We can look at your blog and get a better understanding of what the values on the printout signify.
Thanks for another great article.
Sure it can serve.
The goal is to make hive a good repository for knowledge acquisition. Doing my part from the medical and health angle as always 😊.
Thanks for reaching out @agmoore . Your comments are always top notch.
https://twitter.com/A_G_Moore/status/1557562600346509314
The rewards earned on this comment will go directly to the people( @agmoore ) sharing the post on Twitter as long as they are registered with @poshtoken. Sign up at https://hiveposh.com.
This was really worth reading.
I have done this posting both class lecture and practical but it felt good to be reminded cause sincerely I have forgotten some of them and some I didn't understand very well, but this has cleared a lot of things.
Thanks for this once again.
Indeed it feels good. Most of what we learn ij school, over time, we begin to naturally prune some unnecessary info's because we tend to have less use for them due to specialization.